Anterior Approach
 Incision
Incision
 Spinal Preparation
Spinal Preparation
 Screw & Rod Placement
Screw & Rod Placement
 Fusion
Fusion
What is it?
There are several different approaches that a surgeon will use to correct spinal deformity such as scoliosis and kyphosis, including the traditional posterior approach, an anterior approach, or both. The anterior approach to scoliosis means that the surgeon will approach the spinal column from the front of the spine rather than through the back.
Technically speaking, the actual surgical incision and approach to the spine is through the side of the chest or abdomen (stomach area) rather than down the front of your body, as many patients would envision it. The anterior approach allows surgeons to remove discs from the front of the spine, place corrective spinal instrumentation and perform a spinal fusion.
Why is it done?
The choice of an open anterior approach to the spine is based on a number of different factors including the type of scoliosis, location of the curvature of spine, ease of approach to the area of the curve, and the preference of the surgeon. There are certain types of scoliosis curves, such as those involving the thoracolumbar spine, that are especially amenable to the anterior approach. The surgeon may be able to fuse a shorter segment of the spine using the anterior approach, preserving more motion in the spinal column.
Anterior instrumentation techniques can produce very powerful correction of spinal deformities. However, this approach is more difficult than the standard posterior approach.
The Operation
The first thing that happens after you enter the operating room is that your anesthesiologist will help you to fall asleep. Once you are completely asleep, the anesthesiologist will place a breathing tube to assist with your breathing during surgery, establish a variety of catheters in your veins, and often an arterial catheter in your wrist, all of which allow for monitoring of heart function, blood pressure, fluid status, and the depth of anesthesia during your operation. This allows the anesthesiologist to be sure that you remain completely asleep during the operation. Once this is completed, the patient is rolled onto their side, with the operative side facing up, into what is termed the "lateral decubitus position."
Incision
The incision is made on the patient's side. Depending on the part of the spine that requires correction, this may be over the chest wall or lower down along the abdomen. The surgeon deflates the lung and removes a rib in order to reach the spine. Most patients find it interesting that the rib will grow back over time, especially if you are young. For lower incisions, the surgeon may need to detach the diaphragm to gain access to the spine, especially for thoracolumbar curves and those in the lumbar spine.
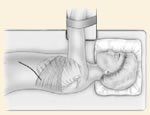
Spinal Preparation
Once the surface of the spinal column is exposed, the surgeon will often remove the disc material from between the vertebra involved in the curve. This will increase the flexibility of the curve and provide a large surface area for spinal fusion. Disc removal is an important adjunct to the anterior correction of scoliosis.
Screw and Rod Placement
Placing instrumentation in the front of the spine completes correction of the spinal deformity. This usually consists of placing a vertebral body screw at each vertebral level involved in the curve. These screws are then attached to a single or double rod at each level. A combination of compression along the rod, and rotation of the rod will produce correction of the spinal deformity.
Fusion
After the final adjustment and tightening of the instrumentation, a fusion is performed. The bony surface between the vertebral bodies is roughened and bone graft is packed into the space between the vertebral bodies. There are a variety of different sources for bone graft including the removed rib, the crest of the pelvis, allograft bone, and other bone substitutes.
Incision Closure
The incision is closed and dressed. If the surgeon has been in the chest cavity, then it will be necessary to place a chest tube through the side of the chest to help keep you lung expanded after the surgery. |


